Everyone agrees that health care is bankrupting the nation. The prevailing winds have carried the argument that a system that pays per unit of health care delivered and thus favors volume over value is responsible. The problem, you see, was the doctors. They were just incentivized to do too much. This incontrovertible fact was the basis for changes in the healthcare system that favored hospital employment and have made the salaried physician the new normal. Yet healthcare costs remain ascendant.
Why?
It turns out overutilization in the US healthcare system isn’t what its cracked up to be.
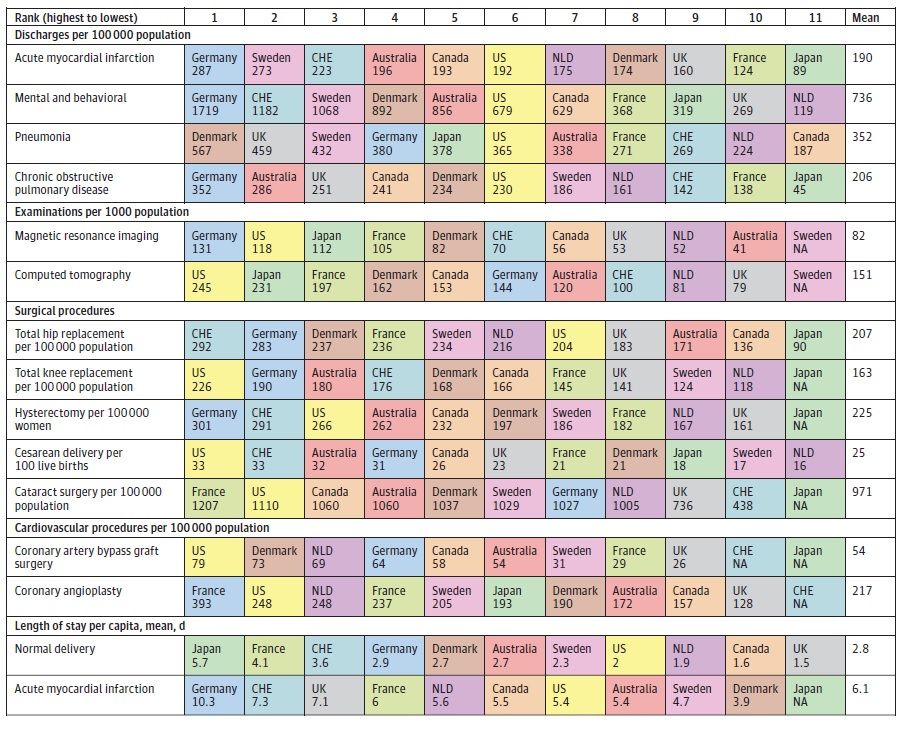
Figure 1
A recent analysis (Figure 1) by Papanicolas et al., in JAMA demonstrates that while the United states is no slouch with regards to volume of imaging and procedures in a variety of different categories, it does not explain a health care system twice as expensive as its nearest competitor. The problem turns out not to be volume, rather its the unit price of healthcare in the United States.
Health care costs and glass houses
There are many stones cast by all the various players in healthcare when it comes to cost, and of course everyone bears some degree of responsibility, but its also clear that some folks live in larger glass houses than others. The most beautiful of all the glass houses are those built by hospitals. From 1996 to 2013, it was not population growth, health status, doctors visits, or prescription drugs that drove spending increases. Sixty-three percent of the increase in cost over an almost 20 year time span can be attributed to hospital stays and testing during doctor visits. Consider that the average hospital stay in the US costs $18,142, and lasts 4.9 days compared to other industrialized countries where average hospital stays last 7.7 days, and cost $6,222. But despite these exorbitant prices hospital systems in the United States complain they barely stay afloat.
Physicians blame administrators, administrators blame physicians, woke liberal venture capitalists blame the Koch Brothers, and economists blame everyone. Ambling through hospitals for the better part of the last two decades suggests real culpability strikes disturbingly close to home. Physicians work in a hospital climate where they are utterly oblivious to the cost of the health care they deliver. No one has any idea what an xray, a bag of saline, or an antibiotic costs. Insulation from cost isn’t all bad – it’s nice to know physician decisions are being made irrespective of the ability to pay, but the flip side of this is that there is precious little incentive to be efficient about health care delivery. Physicians ask for the moon, and usually get it. Hospital administrators poorly versed in clinical matters respond to high costs by doing what they do best: pushing doctors to see as many patients as possible, and rewarding physician rain makers that bring in the most clinical revenue. So, hospital administrators don’t choose to run inefficient enterprises, they just happen to be constrained by clinical partners with no incentive to be remotely efficient.
Consider the change over time in how hospitals are staffed. It used to be that hospitals were staging grounds for physicians who owned and operated their practices, managing busy outpatient clinics, and managing patients in the hospital when the need arose. In this setup, the hospital had no role in paying physicians directly, rather physicians paid themselves out of the clinical revenue generated from seeing the patient in the hospital. Driven by a system that moved to pay hospitals per diagnosis rather than by number of days, and thus put a premium on shortening the length of stay, the inpatient hospitalist was born. Hospitalists are physicians who specialize in the care of hospitalized patient and are almost always employed by hospitals. It soon became standard for outpatient physicians to stay in clinics, and have hospitalists take care of inpatients. In theory, this would allow for better care of inpatients, and allow primary care physicians to see more outpatients. In the real world, as the outpatient practice of medicine was made more onerous and less lucrative, doctors flocked to do hospital shift work upon graduating.
The results in hospitals were wondrous to behold. The same small hospital I frequented that a decade prior operated with a skeleton full time physician crew now employs over 20 full time hospitalists. Length of stays are certainly shorter, documentation of inpatient stays is robust, but of course, there is no evidence that real outcomes for patients are any better. Hospitalists initially were focused within general internal medicine, but have now quickly metastasized to specialty care as well. Innovation in hospitals seems to consist of creating a fresh class of hospitalists for every organ system. Soon there will be hospitalists that specialize only in the big toe. The documentation promises to be fantastic. Factoring in medical malpractice and benefits, the average hospitalist in a big city market costs a quarter million dollars yearly today, and there are 50,000 hospitalists now working in the United States. All of this contributes to hospital salt water that is the most expensive in human history. To be absolutely clear, I am not suggesting there is no value to hospitalists. Some of the best physicians I know belong to this group. I am suggesting that this is an utterly inefficient, fragmented way to deliver care supported by health care prices outside the bounds of reality.
Using the evidence to compound health care costs
And this is only the tip of the iceberg. Hospitals are masterful in their ability to expend vast resources to achieve illusory goals. In all fairness, this is driven by a research industrial complex constantly publishing the next great therapies that may happen to reach statistical significance, but in reality have at most Lilliputian effect sizes.
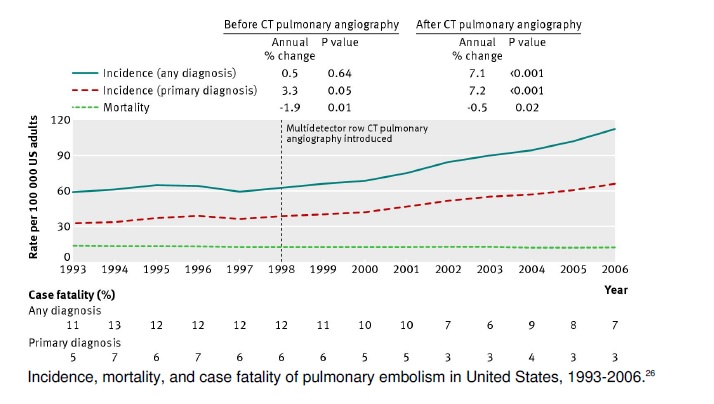
Consider a recent multidisciplinary ‘teaching’ conference I happened to attend that was focused on the management of pulmonary embolism (clots in the lung). The most important thing to know about pulmonary embolisms is what was not mentioned during the conference – the case fatality rate for the diagnosis has not changed in a quarter century. The chart below does demonstrate a doubling of the incidence of PE, but this would be entirely because of ever more sensitive ways to image the pulmonary arteries that reveal clinically irrelevant pathology since there has been no change in deaths from PE over the same time span!
Nonetheless, this particular academic conference has interventional radiologists, cardiologists, pulmonary critical care doctors, vascular medicine physicians, and yes even hospitalists impressively arrayed to focus on improving the management of Pulmonary Embolism. The propose of this conference is to make a rare problem even rarer by creating a hospital Avengers team know as PERT (Pulmonary Embolism Response Team). The goal of the meeting is to convince the wider medical community to activate the PERT team to evaluate pulmonary embolisms for new therapies for PE.
Traditionally PE’s are treated with blood thinners (Heparin/low molecular weight heparin/Factor Xa inhibitors) that prevent propagation of clot or clot busting drugs that actually break down clot. A very small number of patients don’t respond to these therapies because the burden of clot in the lungs is too great, and the thrombus needs to be surgically removed in a gory, but life saving maneuver called a pulmonary thrombectomy.
More recently, interventional radiologists have developed techniques to thread catheters directly into the pulmonary arteries to dissolve clots – a technique known as catheter directed thrombolysis (CDT). The clear message at the conference was that your next patient with a pulmonary embolism should be evaluated by the PE response team for advanced therapies such as these. The basis for all of this is sold as evidence based commandments, but the reality is far from it. (Readers are advised to skip the next two paragraphs if they are allergic to the technical details)
The results of this approach are somewhat predictable, and are encapsulated in an interesting paper described a single institutions experience with PERT. The study looked at a 20 month time window after PERT came to a New York Hospital. There were a total of 124 PERT activations – 43 in the first ten months, 81 in the last ten months. 21/25 patients taken for CDT were taken because of something called submassive PE. Submassive PE refers to strain seen on the right side of the heart as it attempts to pump blood around the clot. It used to be that right sided strain was diagnosed based on a heart ultrasound, but recently a more sensitive, but less specific technique measuring proteins released by the straining right heart were included as part of the diagnostic criteria. The problem is that this biomarker elevation without sonographic evidence of right ventricular dysfunction isn’t a high risk marker in isolation because any stretch of the ventricular chambers will cause some leakage of biomarkers. Only 13-14% who had an abnormal test in a case series ended up dying. While this is not a small number, it does argue against this test in isolation being able to discriminate a population that would significantly benefit from an intervention. Even if you add in the presence of sonographic right ventricular dysfunction, it is unclear that using clot busting medications up front is beneficial. A 2003 study that compared a clot busting drug to blood thinning was ‘positive’ only because more people in the blood thinning arm eventually ended up getting a clot busting drug. The PEITHO trial in 2014 showed similar results. More patients clinically decompensated in the blood thinning only group (5.6% vs 2.6%) but overall survival was no different between the two groups, though there were more bleeds into the brain (2% vs 0.2%) with clot busting drug. So, in general, a strategy of blood thinning first with addition of a clot buster in the case of clinical decompensation is a safe yet effective option.
CDT sought to capture the small benefit of systemic thrombolysis while reducing the risk of bleeding into the brain by infusing clot busting drug directly into the artery where the clot resides. The SEATTLE II trial examine this strategy by taking 150 patients with central PE and performing CDT. Statistically significant differences were seen before and after CDT with regards to pulmonary artery pressures, and left to right chamber size ratio. I don’t mind relevant surrogate endpoints, but the problem here is that the clinical meaningfulness of these surrogate endpoints is questionable.. Pulmonary artery pressures as well as right ventricular chamber size are notoriously dynamic in nature. Transient elevations in pulmonary artery pressures cause the thin walled, compliant right ventricle to dilate frequently. Both parameters may quickly return to normal once the underlying cause of high pulmonary pressures has been treated. There was also no control arm to see how CDT performed relative to conventional blood thinning. The trial certainly did demonstrate safety, but was far from convincing in demonstrating efficacy.
To be clear, I’m a fan of procedures with a large upside and little downside in patients in extremis. I don’t care that much about negative randomized control trials in this space because I don’t really care about average yardage gained when throwing a hail mary. But we all should care when protocols are put in place to trigger algorithms in patients that aren’t in extremis. This is usually what happens when a panel comes together to design protocols. In order for them to be practical, they are usually simple flow diagrams based on some easy to measure variable. You can’t have a protocol that says “if patient looks sick” because that would be subjective and introduce that horror of all horrors : variability. Judgement is deferred to the PERT team that is more likely than not to be comprised of someone making a decision based on reading some other disconnected from the case physician report of an echocardiogram. That this is state-of-the art medical care in 2018 would make Osler weep.
The change in practice pattern after PERT institution are remarkably predictable. If you set up a protocol to call a barber, you get a lot of haircuts. In the 20 months prior to PERT there was 1 CDT. In the 20 months after PERT inception, there were 25. Recall the problem we are attempting to solve (Death related to PE) has a rare case fatality rate that has not changed in two decades. The majority of these PERT activations were due solely to the presence of a biomarker elevation, which almost surely means most of these interventions took place in patients that would likely have been fine with conventional anticoagulant therapy.
My bias, and unwillingness to trust the surrogate endpoint improvement relates to the large number of patients who develop transient RV dysfunction during an acute event that normalizes after conventional therapy. There are a small minority of individuals who develop chronic clot and elevated pressures, but it is impossible with what we know now to predict who that is, and we don’t have a good sense either mechanistically or in a trial setting if CDT would prevent this. So while it is wonderful to know there is another option for the decompensating patient with a PE, the PERT program appears designed to funnel more patients to a lab to get a procedure with questionable benefit.
The resources to marshall all of this are not cheap. A separate layer of PERT consult physicians are added to the mix, catheters to do the procedure need to be stocked, and staffing to accommodate 24/7 interventional radiology coverage for this procedure are marshalled. Outside community hospitals in the network even start to send patients to the hub just to have this procedure.
Costs spiral, physicians pat themselves on the back, patients thank the heavens their lives were saved, and hospital executives earnestly proclaim to politicians and those who pay for healthcare that providing state of the art healthcare in the United States is an expensive endeavor they can do nothing about.Physicians are wont to point everywhere but themselves whenever high prices in health care are raised. I know all the arguments well, but the hard truth lurking beneath the covers is that physicians lie at the heart of all of this. Fixing this mess from the bottom up will require physicians to take ownership of a siuation we have created lest we wish the solution be dictated to us by people without a clue.
The cartoonist Walt Kelley said it best : “We have met the enemy and he is us”.
